Printable Form Cms 1763
Printable Form Cms 1763 - Request for termination of premium hospital an/or supplementary medical insurance keywords: Either way, you will have to enlist the testimony of two witnesses who must assure the finished form before submission. Check the box beside the type of coverage you wish to terminate. If another person is executing the request, write the name beneath the enrollee’s name. If you have plan a, this means you’re terminating your hospital insurance. Premium hospita, supplementary medical insurance created date: Go to the chrome web store and add the signnow extension to your browser. What happens next depends on why you’re canceling your part b coverage. Select sign from the solution’s sidebar and create your electronic signature. Select the form you want in the library of templates. Web please hold emails during this time and send on september 6. If you’re enrolled in original. Go to the chrome web store and add the signnow extension to your browser. This is a standard department of health and human services form it is for use by any medicare enrollee who wants to stop receiving premium hospital (medicare. Open the form in our online editing tool. Log in to your account. Request for termination of premium hospital an/or supplementary medical insurance keywords: Premium hospita, supplementary medical insurance created date: Open the email you received with the documents that need signing. Web cms 1763 request for termination of premium hospital an/or supplementary medical insurance author: Web cms 1763 request for termination of premium hospital an/or supplementary medical insurance author: You’ll need to have a personal interview with social security before you can terminate your medicare part b coverage. Once completed you can sign your fillable form or send for signing. Request for termination of premium hospital an/or supplementary medical insurance keywords: The centers for medicare. If another person is executing the request, write the name beneath the enrollee’s name. All you need is smooth internet connection and a device to work on. Web cms 1763 request for termination of premium hospital an/or supplementary medical insurance author: All forms are printable and downloadable. This form is used to terminate the hospital and or medical insurance benefits. Select the form you want in the library of templates. If another person is executing the request, write the name beneath the enrollee’s name. Check the box beside the type of coverage you wish to terminate. Request for termination of premium hospital an/or supplementary medical insurance keywords: Open the form in our online editing tool. If another person is executing the request, write the name beneath the enrollee’s name. Request for termination of premium hospital an/or supplementary medical insurance keywords: Log in to your account. Web below are five simple steps to get your cms 1763 form designed without leaving your gmail account: Section 1838(b) and 1818a(c)(2)(b) of the social security act require filing of. All you need is smooth internet connection and a device to work on. You must complete this form during an interview with a social security representative; You can do this either during a personal interview at a social security office or on the phone. Web cms 1763 request for termination of premium hospital an/or supplementary medical insurance author: Log in. Premium hospita, supplementary medical insurance created date: Web however, you may need to have a personal interview with social security to review the risks of dropping coverage and to assist you with your request. Premium hospita, supplementary medical insurance created date: If another person is executing the request, write the name beneath the enrollee’s name. Log in to your account. If you have plan a, this means you’re terminating your hospital insurance. The centers for medicare & medicaid services (cms) is a federal agency within the u.s. Either way, you will have to enlist the testimony of two witnesses who must assure the finished form before submission. Web form approved omb no. Complete all necessary information in the necessary fillable fields. Web please hold emails during this time and send on september 6. Signnow combines ease of use, affordability and security in one online tool, all without forcing extra ddd on you. All you need is smooth internet connection and a device to work on. Web stick to these simple instructions to get cms 1763 ready for submitting: What happens next depends on why you’re canceling your part b coverage. Use fill to complete blank online medicare & medicaid pdf forms for free.
Form CMS10106 Download Fillable PDF or Fill Online 1800medicare

Free Printable 1500 Medical Claim Form Printable Form, Templates and

Medicare Part B Form Cms 1763 Form Resume Examples lV8NWx7V10
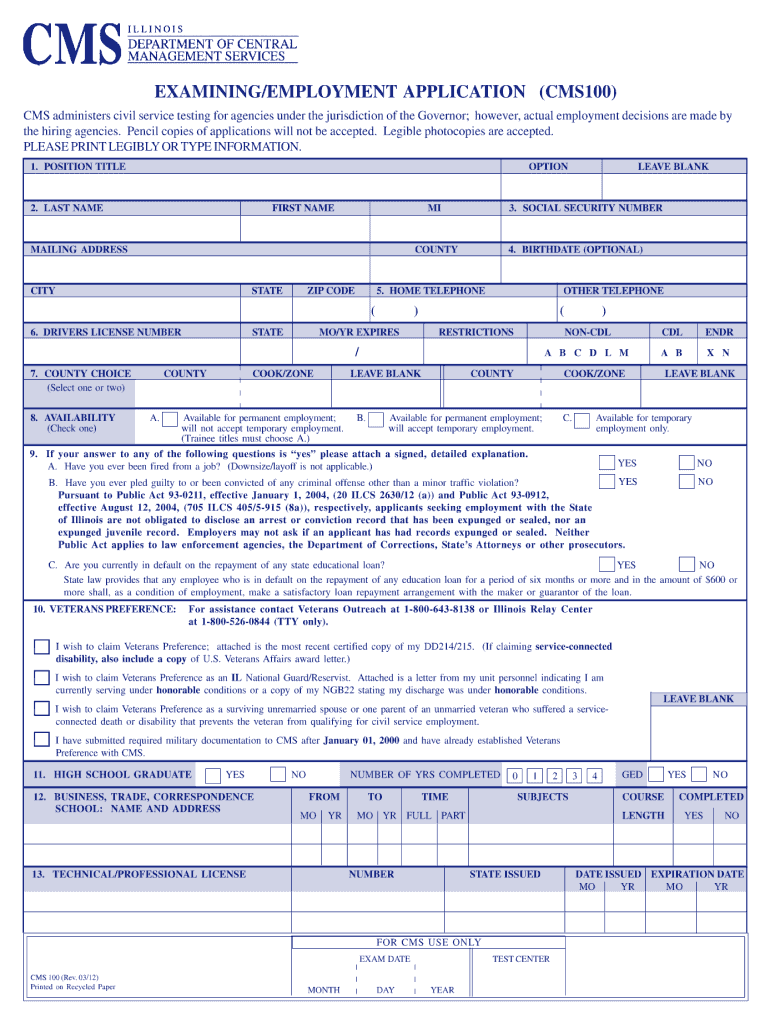
IL CMS 100 20122021 Fill and Sign Printable Template Online US
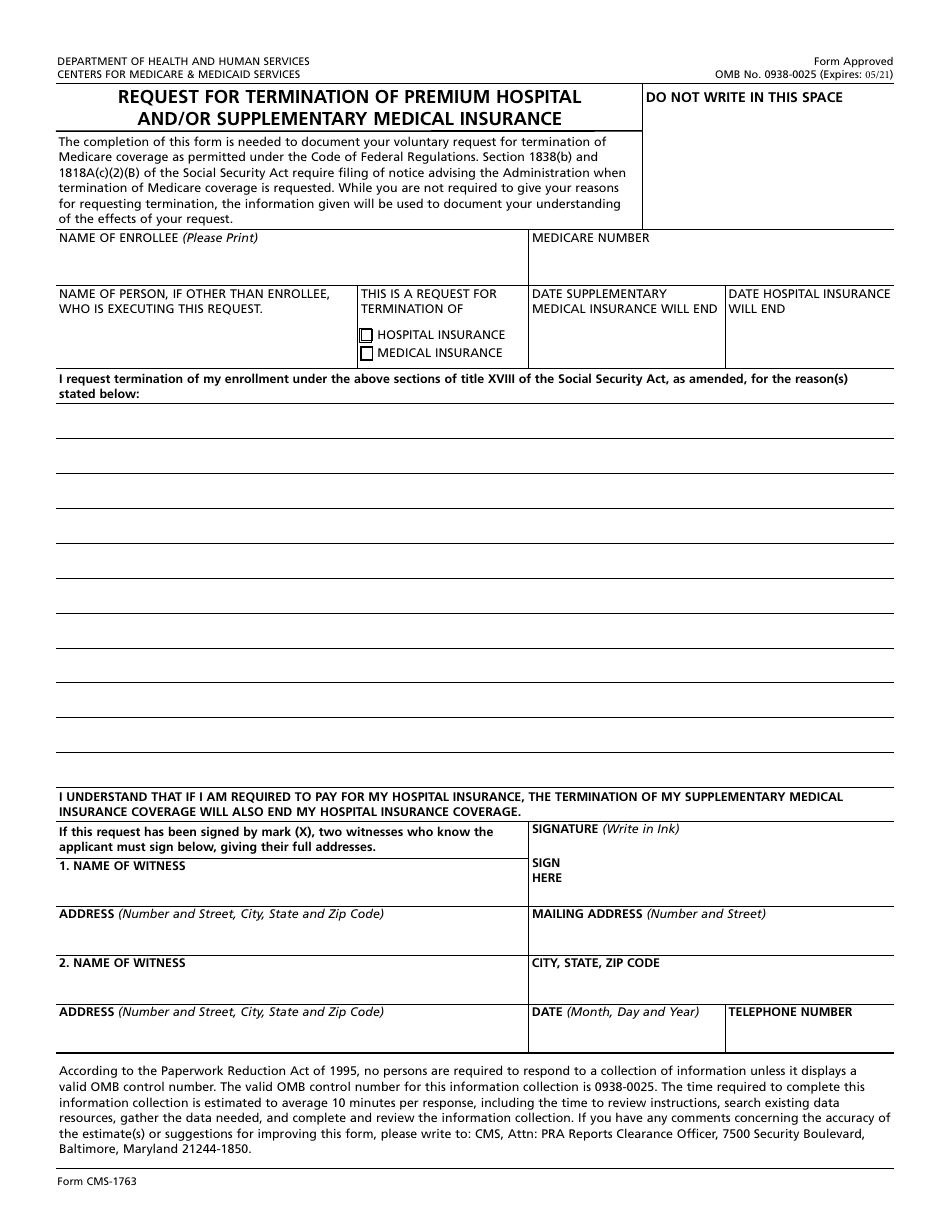
Form CMS1763 Download Fillable PDF or Fill Online Request for
Open The Email You Received With The Documents That Need Signing.
According To Statistics, About 14,000 Citizens Initiate This Form Completion.
You Can Do This Either During A Personal Interview At A Social Security Office Or On The Phone.
If You’re Enrolled In Original.
Related Post: