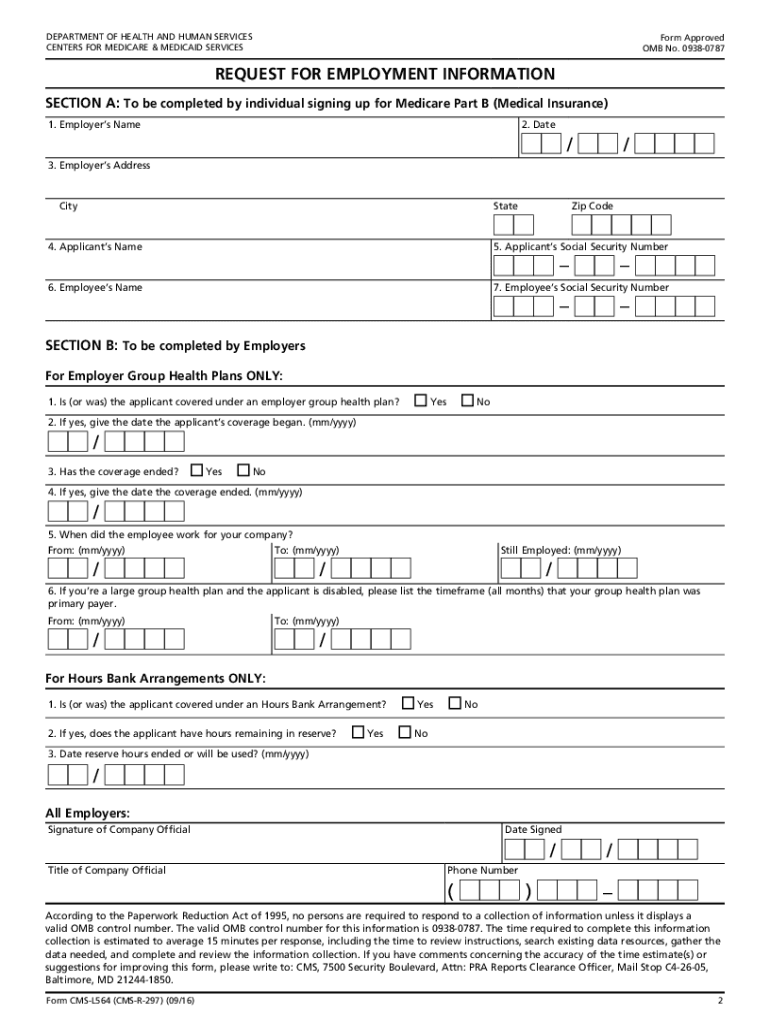
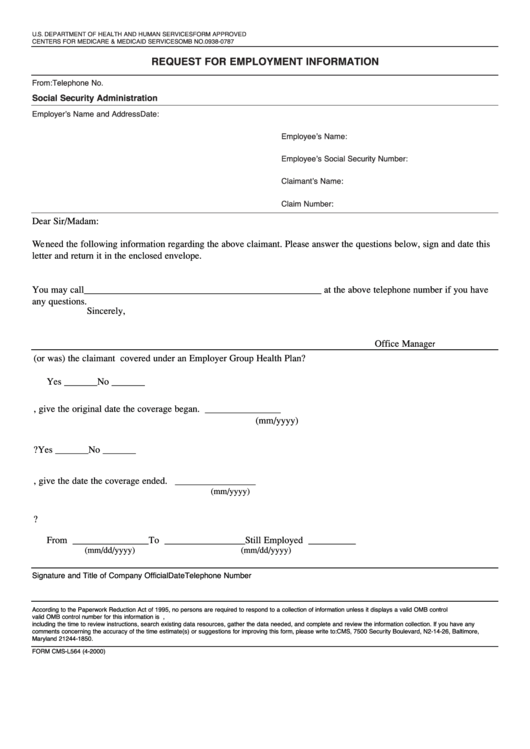
Cms L564 Printable Form
Cms L564 Printable Form - You retired within the last 8 months. Write the name of your employer. Write the date that you’re filling out the request for employment information form. Social security administration telephone number: Department of health and human services centers for medicare & medicaid services form approved omb no. The person applying for medicare completes all of section a. Web form cms l564/r297 (08/20) 2 fform approved omb no. The person applying for medicare completes all of section a. To be completed by individual signing up for medicare part b (medical insurance) 1. If you delayed enrolling in medicare because you had coverage through your job, use this form to enroll during your special enrollment period (sep). If you delayed enrolling in medicare because you had coverage through your job, use this form to enroll during your special enrollment period (sep). You retired within the last 8 months. Write the date that you’re filling out the request for employment information form. The person applying for medicare completes all of section a. Giving the social security administration proof you’re eligible to sign up for part b if: Department of health and human services centers for medicare & medicaid services form approved omb no. Social security administration telephone number: Write the name of your employer. Write the date that you’re filling out the request for employment. Web form cms l564/r297 (08/20) 2 fform approved omb no. Write the name of your employer. Write the name of your employer. Write the date that you’re filling out the request for employment. Social security administration telephone number: Giving the social security administration proof you’re eligible to sign up for part b if: Write the name of your employer. Write the date that you’re filling out the request for employment. To be completed by individual signing up for medicare part b (medical insurance) 1. If you delayed enrolling in medicare because you had coverage through your job, use this form to enroll during your special enrollment period (sep). Department of health and human. The person applying for medicare completes all of section a. The person applying for medicare completes all of section a. If you delayed enrolling in medicare because you had coverage through your job, use this form to enroll during your special enrollment period (sep). You retired within the last 8 months. Web form cms l564/r297 (08/20) 2 fform approved omb. To be completed by individual signing up for medicare part b (medical insurance) 1. The person applying for medicare completes all of section a. Write the name of your employer. Social security administration telephone number: Write the date that you’re filling out the request for employment. Department of health and human services centers for medicare & medicaid services form approved omb no. Write the name of your employer. Write the name of your employer. The person applying for medicare completes all of section a. You retired within the last 8 months. Social security administration telephone number: Write the date that you’re filling out the request for employment information form. To be completed by individual signing up for medicare part b (medical insurance) 1. Giving the social security administration proof you’re eligible to sign up for part b if: Department of health and human services centers for medicare & medicaid services form. You retired within the last 8 months. Write the name of your employer. The person applying for medicare completes all of section a. Department of health and human services centers for medicare & medicaid services form approved omb no. The person applying for medicare completes all of section a. Write the name of your employer. Giving the social security administration proof you’re eligible to sign up for part b if: The person applying for medicare completes all of section a. If you delayed enrolling in medicare because you had coverage through your job, use this form to enroll during your special enrollment period (sep). Write the name of your. Write the date that you’re filling out the request for employment. Department of health and human services centers for medicare & medicaid services form approved omb no. Giving the social security administration proof you’re eligible to sign up for part b if: Write the name of your employer. Social security administration telephone number: Write the date that you’re filling out the request for employment. Web form cms l564/r297 (08/20) 2 fform approved omb no. The person applying for medicare completes all of section a. Write the date that you’re filling out the request for employment information form. The person applying for medicare completes all of section a. The person applying for medicare completes all of section a. Write the name of your employer. You retired within the last 8 months. If you delayed enrolling in medicare because you had coverage through your job, use this form to enroll during your special enrollment period (sep). Giving the social security administration proof you’re eligible to sign up for part b if: The person applying for medicare completes all of section a. Write the name of your employer. Write the date that you’re filling out the request for employment. Web form cms l564/r297 (08/20) 2 fform approved omb no. To be completed by individual signing up for medicare part b (medical insurance) 1.
Commercial Loan Application Form Financial Report
CMSL564 2016 Fill and Sign Printable Template Online US Legal Forms
Form CmsL564 Request For Employment Information, Medicare True/false

Gallery of Medicare Part B Enrollment form Cms L564 New 54 Awesome

Medicare Part B Application Form Cms L564 Universal Network
Medicare Part A Application Form Medicare Id Card Sample Inspirational

Cms L564 Printable Form Master of Documents
1990 Form CMS40B Fill Online, Printable, Fillable, Blank pdfFiller

Medicare Part B Application Form Cms L564 Form Resume Examples

2010 Form CMSL564 Fill Online, Printable, Fillable, Blank pdfFiller
Social Security Administration Telephone Number:
Write The Date That You’re Filling Out The Request For Employment Information Form.
Department Of Health And Human Services Centers For Medicare & Medicaid Services Form Approved Omb No.
Related Post: